
We Need a Radically Different Mindset

Intellectuals solve problems, geniuses prevent them.
~ Albert Einstein
By Dr. Rama
The biggest threat to vascular health is atherosclerosis and its main consequence – Atherosclerotic Cardiovascular Disease (ASCVD). As someone who survived a near-fatal NSTEMI (Non-ST Elevation Myocardial Infarction) that required emergency placement of drug-eluting coronary artery stents approximately four weeks ago, I certainly understand the formidable clinical challenge posed by ASCVD. Fortunately, we are living in an age where we are much closer to lasting clinical solutions that will enable us to ARREST & REVERSE clinical atherosclerosis. As a matter of fact, there are remedies that are available today that can achieve these goals. Not many are aware of these remedies. Unfortunately, I have already suffered two Major Adverse Cardiovascular events (MACE) that resulted from clinical atherosclerosis – Intracerebral hemorrhage (ICH) and NSTEMI. Both events could have been prevented. But that is another story for another day.
Currently, I am in the midst of implementing AGGRESSIVE clinical treatment plans that will ARREST & REVERSE clinical atherosclerosis. Embarking on this long and expensive process has been extremely hard and challenging and it involves facing and overcoming formidable barriers and realizing that I am on my own if I want to prevent MACE in the future by ARRESTING & REVERSING clinical atherosclerosis. One of the pharmacological treatment modalities involves switching off the gene that controls the synthesis of a protein that blocks the LDL-C receptors’ binding and uptake of LDL-C (Low-Density Lipoprotein-Cholesterol). This then leads to extremely low levels of LDL-C in the blood. This, along with statin therapy, has been shown in clinical studies to be associated with REVERSAL of clinical atherosclerosis in major blood vessels.
I have been on statin therapy since I experienced ICH and to this, I will soon be adding the pharmacological agent that will be switching off the gene I mentioned earlier. This agent, of course, needs to be administered every sixth month. Soon, there will be a CRISPR-based, base editing therapy that only requires once-in-a-lifetime administration of a pharmacological agent for this problem – i.e., what is popularly called “one and done” therapy.
For a true revolution in health care to take place, we need a radically different mindset and an open mind. For all of us to benefit from the practical use of the exponential rise in the volume of new knowledge in new biology, genomics, and computational medicine, we need to think about human life span more as an ever-changing dynamic process punctuated by unpredictable events and existential challenges to our state of health at any given moment in our life span rather than a static one that is relatively stable during earlier years/phase of life followed by a steady decline in the latter phase/years as we age. From the moment of birth to the time of our death, many challenges and threats to our health arise. Not all of these are within our control. But, with continuing developments in biology, chemistry, and computing many of these clinical problems/diseases can be cured. Case in point: genomic scanning for premature coronary artery disease (CAD) and employing CRISPR-based gene editing therapy to proactively prevent the genetically vulnerable person from developing CAD ever.
This kind of approach requires a mindset that takes a radically different approach to the idea of health. Such an approach is based on the concept that health is a dynamic, homeostatic state, and maintaining it means not just treating diseases after they produce clinical manifestations but also by implementing systematic and truly preventive strategies using proactive genomic scanning for high-risk conditions like ASCVD. This is not my pipe dream. Treatment plans based on this approach are already in clinical use in some medical centers. Imagine for a moment living a life in which the threats of premature CAD or ASCVD are removed/neutralized permanently.
There are, of course, medical, ethical, financial, social, and other concerns in this area that will have to be addressed. In addition, there must be a sustained and systematic emphasis on an optimal diet, regular exercise and sleep and positively proven lifestyle changes. Unfortunately, despite more than a decade of my commitment to these major factors, I was unable to avoid MACE. The only thing I can say about this is that MACE would have been a lot more severe and prolonged had I not implemented these changes nearly a decade ago.
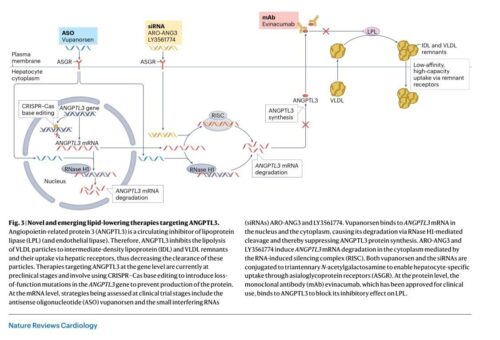
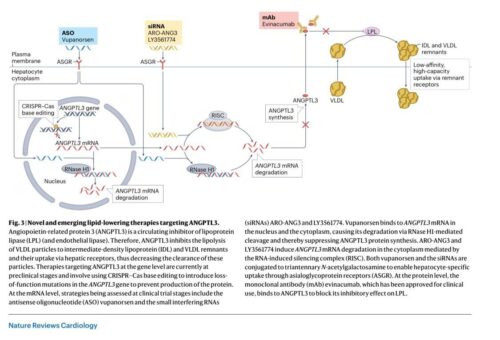
Here are some interesting graphics illustrating recent advances in lipid therapy: (From Julia Brandts and Kausik K. Ray – Nature Reviews Cardiology-2023)
Here is a link (https://www.amjmed.com/article/S0002-9343(20)30945-1/fulltext) to a peer-reviewed paper published in the American Journal of Medicine in 2020 discussing one of the many approaches to reversing clinical atherosclerosis.
I look forward to the day when clinical atherosclerosis is no longer a serious threat to any human being’s vascular health.
Sincerely,
Rama.
_______________________________________________________________________________________________